869
Views & Citations10
Likes & Shares
Marginal fit of the crown is a key assessment of the
fixed partial denture quality. Numerous studies have been performed to evaluate
the marginal fit of CAD/CAM all-ceramic crowns fabricated under ideal
conditions, but very few studies have investigated the impact of real clinical
factors, such as the quality of the abutment preparation. The purpose of this
study is to evaluate the effect of preparation quality on the marginal fit of
CAD/CAM crowns. Fifteen dental clinicians made three preparations of the upper
left first molar on the typodont, and the quality of the preparation was
objectively determined using preparation analyzer software. CAD/CAM crowns were
fabricated using the standard digital workflow on the CEREC System. The
marginal fit of the crown was measured using the Triple-Scan Protocol, and
digitally analyzed and measured in 3D with computer software. Out of 45
prepared abutments, 19 were rated “poor” (PP) and 26 were rated “good” (GP).
The average marginal gap in PP and GP were 82.13 (±9.41) µm and 62.12 (±10.11)
µm, respectively. Statistical analysis with two-tailed t-test showed p-value
< 0.01, indicating significant difference between the two groups. Within the
limitations of this study, the quality of the margin preparation has
significant effect on the marginal fitness of the CAD/CAM all-ceramic crown
Keywords:
Preparation quality, CAD/CAM, Triple scan protocol, Over-mill, Marginal
fitness
Abbreviations:
GP: Good Preparation; PP: Poor Preparation; ME: Marginal Edge; MR: Marginal
Ramp; TSP: Triple Scan Protocol
INTRODUCTION
Recent developments in dental CAD/CAM have vastly improved its
technical maturity, producing restorations that are not only clinically
acceptable and reliable, but cost-effective as well [1]. An abundance of
literature exists that compare the quality and accuracy of restorations
fabricated from conventional workflow versus those from digital procedures. In
general, their conclusions can be split into two groups. Either the studies
concluded that there was no significant difference in quality [2-4], or that
digital workflows are more accurate [5-7].
Fitness of a restoration is a measure of accuracy, and it can be
evaluated by measuring the space between the restoration and the underlying
abutment. McLean et al conducted a 5-year clinical study evaluating marginal
fit of crowns, and determined that marginal gaps up to 120 µm were acceptable
[8]. Several authors also considered marginal gaps between 100 and 150 µm to be
clinically acceptable [9-11]. The source of this large variance in accuracy is
of considerable clinical interest, considering that the resolution of most
dental milling machines is around 25 µm. In an in-vitro study, the authors
compared the marginal gaps of lithium disilicate crowns fabricated by using
three different impressions techniques: one conventional and two digital. The
typodont tooth was prepared extra-orally with a clear guide, and the marginal
gaps of the final crowns were measured using a stereomicroscope. The overall
marginal gaps for conventional and two digital methods were 112.3 µm, 89.8 µm,
and 89.6 µm, respectively [3]. In another study extracted molars were prepared
extra-orally to the recommended reduction guidelines, and the marginal fitness
of their respective CAD/CAM crowns were compared. The study also concluded that
marginal discrepancies in all cases met the clinically-acceptable standard
[12,13]. Similar conclusions can be observed from other similar studies that
compared marginal fitness of CAD/CAM crowns [14,15].
Most of these studies use ideal abutments either prepared extra-orally
or replicated using metal casts. In real clinical situations, ideal
preparations are impractical due to a multitude of environmental, human, and
technical factors. One study that attempted to investigate the human factor
examined the marginal fit of crowns fabricated with the E4Dsystem (PLANMECA,
Finland) and its correlation to the quality of the abutment preparation [16].
The prepared abutments were categorized into “excellent”, “fair”, or “poor”
quality based on visual inspection. In its discussion, the authors admitted to
the possibility of bias and subjectivity with this method. Therefore, the
purpose of this study is to use an objective assessment of preparation quality,
and to investigate whether the preparation quality has a significant effect on
the fitness of the final CAD/CAM crown.
METHOD
Preparation
Fifteen dentists from a teaching hospital, with clinical experiences
ranging from 2 to 18 years, were recruited as subjects of this study. All
participants were given a mandatory 10-minute presentation that reviewed
important preparation parameters. Each participant prepared the same tooth
(#26) on the typodont (Kao Dental GmbH, Germany) three times. The first
preparation was preceded by a 5-minute calibration period, during which the
subjects were able to familiarize themselves with the hardware. All subjects
were provided with identical sets of new burs (Figure 1). In the period between each preparation, the prepared
abutment tooth was removed from the phantom-head and the typodont. The subjects
were not allowed to see the removed teeth until all three preparations were
finished. Once the preparation phase has completed for the subject, the three
abutment teeth were collected, rinsed with tap water, labeled, and stored in
separate containers.
Crown Fabrication
The CEREC Omnicam (Dentsply-Sirona, Germany) was used to create the
digital impression of the prepared abutments. Once the scan data has been
acquired, it was analyzed using the Preparation Analyzer tool to assess the
margin quality of the preparation, which was subsequently categorized into two
groups. If the Preparation Analysis showed no warning, then the preparation is
assigned into the “good preparation” (GP) group. If the software showed one or
more warnings on the margin, then the preparation is designated as “poor
preparation” (PG).
For digital restoration design, the original morphology of the
unprepared tooth was used was used an index. The material selected for
fabrication is the feldspathic porcelain Mark II 14-mm bloc (VITA, Germany),
and all restoration parameters were set to manufacturer’s recommended defaults.
The restorations were milled in the In Lab MCXL (Dentsply-Sirona, Germany)
using extra-fine settings with 12Sburs. The burs were replaced after having
milled 10 crowns. Each crown was visually inspected for milling defects and
re-milled in the off-chance that defects were detected. Then the sprues were
removed and polished via a low-speed hand-piece, and the lumen surfaces
steam-cleaned before trying-in on the abutment.
Analysis
The primary technique used for the data acquisition in 3D marginal fit
analysis is the Triple Scan Protocol (TSP) [17]. In this study, the TRIOS
intra-oral scanner (3Shape, Denmark) was used as the scanner in the protocol.
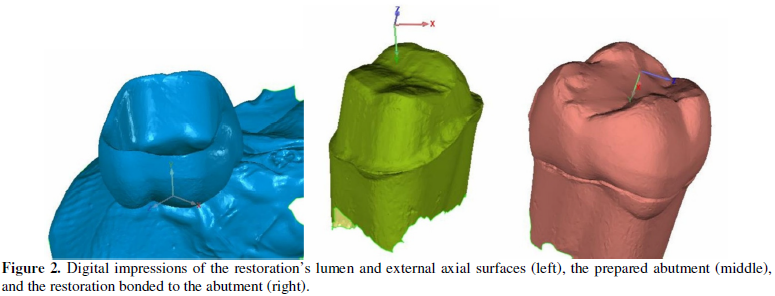
The Triple-Scan Protocol consists of three scans. First, the crown is fixed in
place with beading wax, with the lumen surface facing up and all external axial
surfaces exposed (Scan #1). The TRIOS was then used to scan using
high-resolution mode. The number of 3D image stacks was limited to under 300,
irrespective of the scanning time. After scanning was completed and inspected
in the software for holes, the file was converted and saved into ASCII STL file
format. For the second scan of the protocol, the prepared abutment scanned in a
similar method to the previous step, and the final model was converted into STL
file format (Scan#2). Finally, the third scan of TSP consists of both the crown
and the abutment in their seated positions (Figure 1). Before the scan, the
porcelain crowns were seated onto the abutments with light-body silicone (3M).
Maximum finger pressure was applied for 5 minutes until setting, and entire
specimen was scanned using the same method as the previous steps (Scan #3).
3D Marginal Analysis
Geomagic Studio was used for to create 3D registration of the crown
(Scan #1) and the abutment scan data (Scan #2), using the scan data (Scan #3)
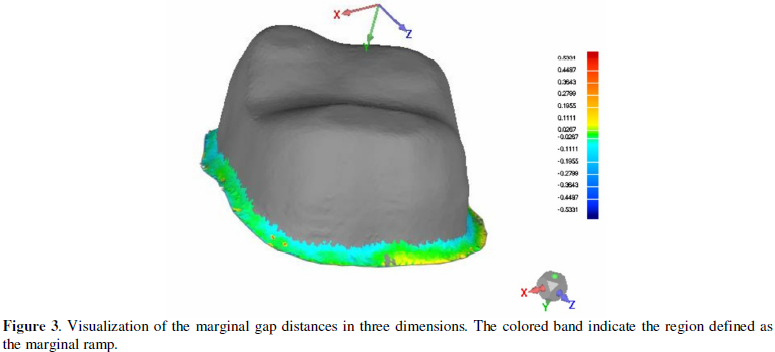
as reference. The margin of the prepared abutment was divided into two regions.
The area from the edge of the margin to the highest curvature before the axial
wall was designated as the marginal ramp (MR) (Figure 2). The outer band of MR consisting of all mesh triangles in
contact with the edge boundary was designated as the marginal edge (ME). Once
these two regions were specified on the abutment, their average distance to the
lumen side of the corresponding crown model can be determined using standard
software functions. For each region, the mean and maximum distances across all
sampling points were calculated.
RESULTS
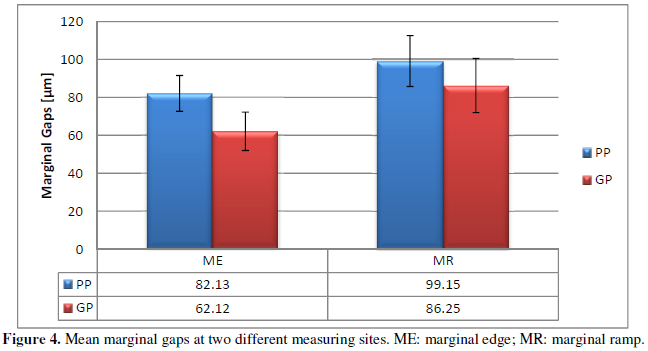
The numbers of samples in PP and PG groups were 19 and 26,
respectively. The mean gap measurements using data acquired from TSP were as
followed; For ME, the mean gap size for PP was 82.13 µm (±9.41), while the mean
gap size for GP was 62.12 µm (±10.11). For MR, the mean gap size for PP was
99.15 µm(±13.46), while the mean gap size for GP was 86.25 µm (±14.23) (Figure 3). No samples were rejected
during inspection.
STATISTICAL ANALYSIS
The results for data from ME and MR indicated statistical significance
(p < 0.01) between PP and GP values. For ME results, the t-score was 6.82
with 43 degrees of freedom. For MR results, the t-score was 2.87 with 43
degrees of freedom.
DISCUSSION
For CAD/CAM restorations, marginal fitness is often of primary concern
because it directly correlates to the long-term health of the dentition and the
surrounding tissue [13,18,19]. Marginal fitness, or discrepancy, is defined as the
“vertical dimension from the finish line of the preparation to the margin of
the restoration” [20]. Poor marginal adaptation of the restoration can increase
micro leakage and plaque accumulation, leading to cement dissolution, secondary
caries, and periodontal disease [21]. There is, however, no clear guideline for
clinically acceptable marginal fit. Christensen [22] considered 39 µm to be the
acceptable marginal discrepancy according to the linear regression prediction
formula. Several authors also considered marginal discrepancies between 100 and
150 µm to be clinically acceptable [8-11].
While digital workflows have shown to produce clinically acceptable
margins [3,12,13], these kinds of studies mostly utilize abutments that were
optimally prepared in-vitro. Ucar et al. [23] used machined steel dies to
evaluate the internal fitness of laser-sintered crowns. Seker et al. [1] and
Baig et al. [15] prepared extracted premolars with a uniform 1 mm rounded
shoulder margin to evaluate marginal fit of CAD/CAM restorations. These studies
failed to capture the inevitable variance caused by human error. In a real
clinical setting, factors such as poor viewing angles, inadequate lighting,
mouth opening limitations, and the skills of the dentist can potentially cause
teeth preparations to become suboptimal. Therefore, the results from these
previous studies represent the best-case scenarios that are very unlikely to
occur.
Since in practice, dentists are able to detect gaps at only the margins
with a dental probe [22], the criteria for preparation quality in this study is
limited to the marginal area. In this study, the average gaps at ME for the PP
and PG groups were 82.13 µm and 62.12 µm, respectively. The ME marks the band
of area directly adjacent to the edge of the finish line, and the gap values in
this study were all within the clinically acceptable value of 120 µm [8].
Furthermore, they are also in agreement with other similar studies that used
intra-oral scanners to fabricate single crown restorations [13,15,24-26].
According to a systemic review [27], which performed a meta-analysis on the
evaluation of marginal fit of single-unit full coverage ceramic restorations,
the mean value of the marginal fit for in-vitro restorations fabricated after
digital impressions was 63.3 µm(95% CI: 50.5–76.0 µm). Considering that these
studies used optimally prepared abutments under controlled settings, the
marginal fitness obtained for the GP group in this study (62.12 µm) is very
close to the value obtained in the systemic review. This seems to suggest that
if the marginal preparation is of sufficiently quality, then near-optimal
marginal fitness can be achieved. On the other hand, if there are areas of
roughness or acute angles that can be detected by the analysis software, then
these imperfections are transferred to the fitness of the final crown.
The software used for preparation quality assessment, Preparation
Analysis, is a simplified version of prep Check (Dentsply-Sirona). It checks
the curvature process of the preparation margin, and if the margin exceeds a
determined section length of a predefined curvature, the region is highlighted
as a warning. The predefined curvature can be indentations or protrusions, and
it is correlated to the milling process. The marginal fit of the CAD/CAM crown
is dependent on how accurately the milling device can reproduce the contours of
the preparation. Since milling is performed with burs, the radius of the bur
poses a physical limitation on how fine a detail can be milled. Therefore, small
features or contours smaller (i.e. rough surfaces, sharp angles) cannot be
perfectly reproduced. When this problem is encountered during the milling
pathway analysis, there are two options for the software algorithm. First, to
ensure complete seating of the crown, the software will generate a milling path
that guarantees milling of all surface features.
This is called over-milling [28], and it necessitates the creation of
extra cement space around the problem region as a compromise. The alternative
method is to simply ignore the geometries that cannot be milled, and instead
favor the preservation of crown integrity. This is called under-milling, and it
can potentially cause an inability for the crown to completely seat. For the
marginal regions with severe enough roughness, either milling strategy will
result in increased marginal gaps.
In a study, researchers fabricated 75 crowns based on abutments of
varied preparation quality determined by visual inspection [16]. The study
concluded that preparation quality has a significant effect on marginal gap
when using chair side CAD/CAM systems and that common error in preparation
design had a negative impact on the mean marginal gap. While our results
concur, the determination of quality by visual inspection was subject to
potential bias. In fact, several other studies have evaluated the intra-rater
variability for the assessment of dental preparation quality, and found the
intra-rater agreement to be between 0.53 and 0.68 [29,30], representing up to
22% variance in binary pass/fail decisions [31]. In contrast, our study uses
the built-in preparation analysis tool (Dentsply-Sirona, Germany) to
objectively evaluate the quality of the preparation.
The methods of evaluating the crown fitness have been well established
in literature. For marginal fit, studies have used the optical microscope
[1,13,15,32-35], scanning electron microscope [1,33,34] or silicone replica
[4,13,14], [16,21,25,32,36]. According a systemic review by Nawafleh et al.
[37], the direct-viewing technique (i.e. microscopes) is the most common method
of studying marginal fitness, accounting for 47.5% of the 183 papers reviewed
in the study. The study concluded that the there was a substantial lack of
consensus relating to marginal adaptation of various crowns, because of the
large variance 0in the results obtained. The silicone replica method, or any
embed-then-section methods [24], for measuring marginal and internal fitness
suffers from one major flaw: using a 2D method to analyze 3D metrics. A recent
study by Kuhn et al. [38] compares analog and digital quantitative and
qualitative analysis for the fit of dental copings, and concluded that the
analog 2D replica technique revealed a loss of information due to the cutting
process. In order to maximize the retention of data, our study employed TSP and
digital software analysis for true 3D measurement.
Recently the Triple-Scan Protocol (TSP) was described and validated for
the fitting accuracy assessment of cast metallic frameworks, titanium copings, and
lithium disilicate partial crowns [17]. This protocol allows for the virtual
registration of two scanned models (abutment and crown) in relation to the
third reference model (crown bonded to abutment). The TSP is non-destructive
and eliminates a great number of shortcomings of 2D fitting accuracy assessment
techniques that have been applied routinely in other studies.
In a study by Boitelle that used the TSP methodology to evaluate 3D
fitting accuracy of CAD/CAM copings, the marginal and internal fitness of the
restoration was divided into three regions [39]. Using the height of the
abutment as the reference, the abutment was separated into the marginal (bottom
15%), the occlusal (top 15%), and the axial (middle 70%) zones. While this
strategy provided a quick method to differentiate various aspects of the
abutment, it would only be useful if the prepared abutment was both axially and
radially symmetrical. Since the teeth were prepared by real clinicians in our
study, the height and width of the margin were highly variable. Therefore, our
study used the morphology of the abutment to delineate different regions. The
mean gap sizes of the marginal area in Boitelle’s study ranged between 54.32 –
66.56 µm, depending on the digital system used, while in our study the
corresponding fitness of the marginal ramp was 86.02 µm.
While the data seems to suggest that even poor-quality preparations can
produce, on average, clinically viable results, these results are only average
values. The presence of variance means that a percentage the margins can
potentially be larger than the acceptable value. The inability for milling
machines to compromise means that there is higher sensitivity to preparation
errors.
CONCLUSIONS
Within the limitations of this study, the following conclusions can be
made:
- There is a significant
difference in the marginal fitness of crowns fabricated from good quality
preparations when compared with those fabricated from poor quality
preparations. Therefore, the null hypothesis is rejected.
- Regardless of preparation quality, the marginal gaps of CAD/CAM crowns were all within the clinically acceptable range.
1.
Şeker E, Ozcelik TB, Rathi N, Yilmaz B (2016) Evaluation of
marginal fit of CAD/CAM restorations fabricated through cone beam
computerized tomography and laboratory scanner data. J Prosthet Dent 115: 47-51.
2.
Berrendero S, Salido MP, Valverde A, Ferreiroa A, Pradíes G
(2016) Influence of conventional and digital intraoral impressions on the fit
of CAD/CAM-fabricated all-ceramic crowns. Clin Oral Investig 20: 2403-2410.
3.
Abdel-Azim T, Rogers K, Elathamna E, Zandinejad A, Metz M, et
al. (2015) Comparison of the marginal fit of lithium disilicate crowns
fabricated with CAD/CAM technology by using conventional impressions and two
intraoral digital scanners. J Prosthet
Dent 114: 554-559.
4.
Ahrberg D, Lauer HC, Ahrberg M, Weigl P (2016) Evaluation of
fit and efficiency of CAD/CAM fabricated all-ceramic restorations based on
direct and indirect digitalization: a double-blinded, randomized clinical
trial. Clin Oral Investig 20:
291-300.
5.
Shembesh M, Ali A, Finkelman M, Weber HP, Zandparsa R (2017) An
In Vitro Comparison of the Marginal Adaptation Accuracy of CAD/CAM Restorations
Using Different Impression Systems: CAD/CAM Marginal Adaptation Accuracy. J Prosthodont 26: 581-586.
6.
Su TS, Sun J (2016) Comparison of marginal and internal fit
of 3-unit ceramic fixed dental prostheses made with either a conventional or
digital impression. J Prosthet Dent 116:
362-367.
7.
Kocaağaoğlu H, Kılınç HI, Albayrak H (2017) Effect of digital
impressions and production protocols on the adaptation of zirconia copings. J Prosthet Dent 117: 102-108.
8.
McLean JW, Von F (1971) The estimation of cement film thickness
by an in vivo technique. Br Dent J 131:
107-111.
9.
Boening KW, Walter MH, Reppel PD (1992) Non-cast titanium
restorations in fixed prosthodontics. J
Oral Rehabil 19: 281-287.
10.
Tsukada G, Tanaka T, Kajihara T, Torii M, Inoue K (2006) Film
thickness and fluidity of various luting cements determined using a trial
indentation meter. Dent Mater 22:
183-188.
11.
Quintas AF, Oliveira F, Bottino MA (2004) Vertical marginal
discrepancy of ceramic copings with different ceramic materials, finish lines,
and luting agents: an in vitro evaluation. J Prosthet Dent 92: 250-257.
12.
Yang X, Lv P, Liu Y, Si W, Feng H (2015) Accuracy of digital
impressions and fitness of single crowns based on digital impressions. Materials 8: 3945-3957.
13.
Ng J, Ruse D, Wyatt C (2014) A comparison of the marginal fit
of crowns fabricated with digital and conventional methods. J Prosthet Dent 112: 555-560.
14.
Colpani JT, Borba M, Della Bona A (2013) Evaluation of
marginal and internal fit of ceramic crown copings. Dent Mater 29: 174-180.
15.
Baig MR, Tan KBC, Nicholls JI (2010) Evaluation of the
marginal fit of a zirconia ceramic computer-aided machined (CAM) crown system. J Prosthet Dent 104: 216-227.
16.
Renne W, McGill ST, Forshee KV, DeFee MR, Mennito AS (2012) Predicting
marginal fit of CAD/CAM crowns based on the presence or absence of common
preparation errors. J Prosthet Dent 108:
310-315.
17.
Holst S, Karl M, Wichmann M, Matta RET (2011) A new
triple-scan protocol for 3D fit assessment of dental restorations. Quintessence Int Berl Ger 42: 651-657.
18.
Reich S, Uhlen S, Gozdowski S, Lohbauer U (2011) Measurement
of cement thickness under lithium disilicate crowns using an impression
material technique. Clin Oral Investig
15: 521-526.
19.
Podhorsky A, Rehmann P, Wöstmann B (2015) Tooth preparation
for full-coverage restorations—a literature review. Clin Oral Investig 19: 959-968.
20.
Kokubo Y, Ohkubo C, Tsumita M, Miyashita A, Vult Von Steyern
P, et al. (2005) Clinical marginal and internal gaps of Procera AllCeram
crowns. J Oral Rehabil 32:
526-530.
21.
Huang Z, Zhang L, Zhu J, Zhao Y, Zhang X (2015) Clinical
Marginal and Internal Fit of Crowns Fabricated Using Different CAD/CAM
Technologies. J Prosthodont 24:
291-295.
22.
Christensen GJ (1966) Marginal fit of gold inlay castings. J Prosthet Dent 16: 297-305.
23.
Ucar Y, Akova T, Akyil MS, Brantley WA (2009) Internal fit
evaluation of crowns prepared using a new dental crown fabrication technique:
Laser-sintered Co-Cr crowns. J
Prosthet Dent 102: 253-259.
24.
Pradíes G, Zarauz C, Valverde A, Ferreiroa A, Martínez-Rus F
(2015) Clinical evaluation comparing the fit of all-ceramic crowns obtained
from silicone and digital intraoral impressions based on wavefront sampling
technology. J Dent 43: 201-208.
25.
Brawek PK, Wolfart S, Endres L, Kirsten A, Reich S (2013) The
clinical accuracy of single crowns exclusively fabricated by digital workflow—the
comparison of two systems. Clin Oral
Investig 17: 2119-2125.
26.
Anadioti E, Aquilino SA,
Gratton DG, Holloway JA, Denry I, et
al. (2014) 3D and 2D Marginal Fit of Pressed and CAD/CAM Lithium
Disilicate Crowns Made from Digital and Conventional Impressions. J Prosthodont 23: 610-617.
27.
Tsirogiannis P, Reissmann DR, Heydecke G (2016) Evaluation of
the marginal fit of single-unit, complete-coverage ceramic restorations
fabricated after digital and conventional impressions: A systematic review and
meta-analysis. J Prosthet Dent 116:
328-335.
28.
Renne W, Wolf B, Kessler R, McPherson K, Mennito AS (2015) Evaluation
of the Marginal Fit of CAD/CAM Crowns Fabricated Using Two Different Chairside
CAD/CAM Systems on Preparations of Varying Quality. J Esthet Restor Dent 27: 194-202.
29.
Satterthwaite JD, Grey NJA (2008) Peer-group assessment of
pre-clinical operative skills in restorative dentistry and comparison with
experienced assessors. Eur J Dent Educ
12: 99-102.
30.
Goepferd SJ, Kerber PE (1980) A comparison of two methods for
evaluating primary class II cavity preparations. J Dent Educ 44: 537-542.
31.
Jenkins SM, Dummer PM, Gilmour AS, Edmunds DH, Hicks R, et
al. (1998) Evaluating undergraduate preclinical operative skill; use of a glance
and grade marking system. J Dent
26: 679-684.
32.
Tidehag P, Ottosson K, Sjögren G (2014) Accuracy of Ceramic
Restorations Made Using an In-office Optical Scanning Technique: An \textlessi\textgreaterIn
Vitro\textless/i\textgreater Study. Oper
Dent 39: 308-316.
33.
Bindl A, Mormann WH (2005) Marginal and internal fit of
all-ceramic CAD/CAM crown-copings on chamfer preparations. J Oral Rehabil 32: 441-447.
34.
Oyagüe RC, Sánchez-Jorge MI, Turrión AS (2010) Evaluation of
fit of zirconia posterior bridge structures constructed with different scanning
methods and preparation angles. Odontol
98: 170-172.
35.
Nakamura T, et al.
(2005) In vitro study on marginal and internal fit of CAD/CAM all-ceramic
crowns. Dent Mater J 24:
456-459.
36.
Moldovan O, Luthardt RG, Corcodel N, Rudolph H (2011) Three-dimensional
fit of CAD/CAM-made zirconia copings. Dent Mater 27: 1273-1278.
37.
Nawafleh NA, Mack F, Evans J, Mackay J, Hatamleh MM (2013) Accuracy
and Reliability of Methods to Measure Marginal Adaptation of Crowns and FDPs: A
Literature Review. J Prosthodont
22: 419-428.
38.
Kuhn K, Ostertag S, Ostertag M, Walter MH, Luthardt RG, et
al. (2015) Comparison of an analog and digital quantitative and qualitative
analysis for the fit of dental copings. Comput
Biol Med 57: 32-41.
39.
Boitelle P, Tapie L, Mawussi B, Fromentin O (2016) 3D fitting
accuracy evaluation of CAD/CAM copings - comparison with spacer design settings.
Int
J Comput Dent 19: 27-43.
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)



